

How To Get Rid Of Sibo
I was recently diagnosed with a severe case of methane SIBO (which I've had for years without realizing that it was causing me to pass a lot more gas than normal) and did a lot of research on what to do about it. By far, the most interesting insights came from about 100 emails plus a 1 hour in-person discussions with Mark Pimentel, who is arguably the world's #1 expert on SIBO.
Quick update: I was cured by single round of antibiotics as described below plus a few weeks on the motility drug, which probably wasn't needed since my motility was fine. How I got SIBO is still a mystery since it is normally due to a motility problem.
The excess gas all went away, but my stomach distention didn't change. So I saw Dr. Linda Nguyen at Stanford who is THE motility expert in the SF bay area. She put me though the standard tests which culminated in a smart pill study. I passed the pill in 24 hours which means I don't have a motility problem. Note: you have to do the imaging studies FIRST because if you have a blockage, the smart pill can get "stuck" requiring emergency surgery to remove. So Linda concluded my abdominal distention was due to abdominal phrenic dyssynergia (APD) which is a condition that is diagnosed by the process of elimination (e.g., since you don't have x,y, and z, then you must have APD). I still haven't found anyone to treat my APD, so reach out to me on LinkedIn using InMail if you can help me!
Because Mark was so generous of his time with me, and because there is so much misinformation on the web about SIBO, I wanted to document the unique insights I learned from him that I didn't find elsewhere in the hopes that it will help others with this condition. I've been told by a number of readers this is the most comprehensive writeup on SIBO on the web. I has 100,000 views with 3,000 claps. So hopefully you will find it useful as well.
I've reviewed the contents of this summary with Mark for accuracy; he thought it was a great addition to the material he's put on the web.
This article is concise because it is written for someone who already knows about the SIBO basics, but has more than likely been horribly misinformed along the way in one or more aspects. So this is like an erratum list for the stuff you've read so far.
Unfortunately, there is a lot of misinformation on SIBO out there (and most physicians do not treat it correctly), so this ended up to be a 28 minute read. But trust me, if you have SIBO, this article will save you both time and money and will be worth the time. Even if you've already read a lot about SIBO, you are almost certain to learn a lot of new info that may lead to a much more successful outcome, with fewer side effects, and, in some cases, substantially lower out of pocket costs.
Here are the most important points:
- SIBO is basically a condition that is, in almost all cases, caused by poor gut motility (failure of the MMC to clean out your small intestine between meals). You cannot get SIBO unless you have a motility problem (except in my case where I had SIBO but my motility was normal showing there are exceptions to every rule). Therefore, in almost all cases, "curing SIBO" is only curing the symptom, not the disease.
- If you don't want it to reoccur, you must find out and fix the root cause of the motility problem. Finding out the root cause means a series of tests which may or may not include physical exam (especially listening to your stomach, upper endoscopy (with biopsies), intestinal MRI and CT scan, smartPill, IB smart blood test, etc). The list of disease states leading to SIBO are listed in Table 1 of Mark's paper referenced below. So if you aren't following a logical process to find the root cause, it's going to keep happening and you'll be stuck on taking a prokinetic each night for a long long time. Finding the root cause is most often a process of hypothesis and eliminating possible causes.
- The 2 "golden rules" in order to get rid of SIBO and minimize recurrence are: 1) take a prokinetic pill and 2) eat discrete meals (for example at 8am, 1pm, and 6pm; ideally at least 4 hours between meals, and you do not want to eat right before bedtime).
- You can "kill your way" out of SIBO with antibiotics, but that is only recommended at the very start to get to remission faster. Fix your motility is key. It's way easier to flush the stuff out with a prokinetic than to kill it.
- In most all cases, until you discover the underlying cause, the only thing you really need is a prokinetic. Mark's favorite for the prokinetic is prucalopride taken at a low dose (typically .5mg each night before bedtime on an empty stomach, but for some can be less or more). For prucalopride, eat nothing for at least 4 hours before taking the pill at bedtime. Then, after taking the pill, try to fast as long as you can before eating something. The longer you fast, the greater the benefit. But don't try to be a hero. There is no award for fasting for all 12 hours and nobody is going to test you and see how you are doing. The drug wears off in 12 hours so no point in fasting longer. Personally, i just eat when I wake up and don't optimize the fasting period. NOTE: Prucalopride is now available in the US (as of April 2019)!
- If you cannot tolerate prucalopride, there are other drug options (mentioned in Table 1 in Mark's paper below): erythromycin and domperidone.
- Using only these the two golden rules in #2 above, most people should be able to completely get rid of SIBO and keep it from recurring; one drug and one eating pattern. Total drug cost (if not covered by insurance): typically a little more than $1/day (if you are clever and buy the 2mg pill and split it into 4 pieces like I do).
- Most people don't know the 2 golden rules, so they relapse, sometimes quickly. I hear stories of people taking multiple rounds of antibiotics then herbs in between the antibiotics. This is insane. You really only should have one round of antibiotics tops, and then the pro-kinetic.
- Mark's Low-Fermentation Diet (LFD) guide is highly useful for understanding SIBO and how the digestive system works. It's a short read, and full of great info and insights you won't find anywhere else. Mark's LFD is much easier to adhere to than any of the other SIBO diets (like SCD and FODMAP diets) because it allows a more options so you don't feel deprived. The whole point of the diet is to identify foods that can be more fully digested and thus minimize bacterial growth. Some foods may not agree with you; avoid them. Some foods may be inappropriate for you, e.g., white bread and rice if you are a diabetic. The foods are simply a list of "relatively safe" foods in general. And you can cheat since the golden rules are the main drivers, not diet. The diet minimizes food for the bacteria if you have not yet addressed the underlying cause of your SIBO. Something is wrong to have caused you to get SIBO in the first place. The LFD is just meant as a stopgap until you discover the root cause of your SIBO. If the root cause is incurable, the the motility is key and the LFD becomes more important. However, if you can restore normal motility overnight through a prokinetic, the LFD is irrelevant since you are fully cleaned out every night. I did the LFD for awhile, but I now eat normally. Absolutely no change in symptoms. So be practical: try the LFD diet and if there are no changes in your symptoms, you have Mark's permission to give it up.
- While you are on the antibiotic regimen, you should ignore the diet. The bacteria are more easily killed when they are replicating so you want to feed them. Mark says, "I have told my patients from day one of rifaximin or treating with antibiotics — and this goes back to the 1980s; this is an old microbiological concept — happy bacteria, happy and well-fed bacteria, are more sensitive to antibiotics and are easier to kill. What that means is that most antibiotics work on the replicating cell wall of bacteria. When bacteria are in hibernation, starving, distressed, they wall off, don't replicate, and they just sit there, waiting for conditions to improve. That's a survival mode. So when the bacteria are in survival mode, antibiotics won't penetrate and won't work as well."
- While you should be able to get rid of SIBO with ONLY a good prokinetic, you may be able to get rid of SIBO faster by starting with a 2 week antibiotic regimen. For methane dominant SIBO, the recommended treatment is 550 Rifaximin ( Xifaxan)+ 250mg Metronidazole (Flagyl) taken 3 times a day for at least 14 days. This is slightly better than the combo with neomycin. Some people get stressed out about not tolerating the drugs. No problem. The antibiotics are optional.
- A lot of people may make the mistake of upping the dosage of prucalopride which may lead to undesirable side effects. Also, note that Prucalopride will induce phase III MMCs only when taken in a fasted state. The whole point of prucalopride is give your intestines an extra "boost" during the longest fast of the day (overnight); therefore for SIBO it is prescribed at 25% of the "standard dosage" because the "standard dosing" for prucalopride is set by the labelled use (chronic idiopathic constipation (CIC)), not for SIBO patients. Personally, I found nearly zero difference in how I feel at .5 mg to 2 mg. So stick with the .5 mg unless you have a good reason to go higher. Always take fasted (>4 hours since last meal), right before bed. In my case, if I eat at 7pm, I'll take the pill at bedtime. Otherwise, if I wake up at night, I'll take the pill. The pill lasts for 12 hours so ideally you should not eat anything (including pills/medication!!) for 12 hours after taking the pill to get the fastest improvement and the most bang for your buck. If you can't last 12 hours, don't sweat it. I'm just citing the ideal. There is no benefit to fasting longer than 12 hours after taking the pill. So far, no side effects whatsoever doing it this way.
- I asked Mark if you can simply flush the bacteria out of your small intestine by drinking a lot of water. NB: A lot of water will kill you so don't do this! He said hydration makes no difference because water is absorbed very quickly so it's not like you have any chance of "flushing" out the bacteria by supplementing with water. The small bowel when spread out is about half the size of a badminton court (previously they thought it was the size of a tennis court).
- You can monitor your progress during treatment by doing "fasting" breath test. No substrate ingestion is required. Just fast overnight, brush your teeth, and take the breath test. This is not super accurate but is reasonably useful to see if you are making solid progress in the right direction as you consume the drugs. See below on the cheat that you can use to do this very economically. But I basically monitor symptoms. Doing "at home" breath tests is really over the top…suitable for analytical types like me and even I don't do it.
- You can NEVER win the war against bacteria by trying to starve it. Bacteria multiply by 2 every 12 hours. So if you could wipe out 99.9% of bacteria with an antibiotic, it will all return in just 5 days. So if you starve the bacteria, the stuff that grows back will be all replicas of the bacteria that is immune to starvation. This is evolution at its finest (especially so if you have methane SIBO; methanogens are very primitive and very hard to kill). This is why all the clever, innovative approaches people have proposed (Iodine, chlorine, ozone, …) are simply never going to work. You won't kill it all and it comes back way too fast. Your ONLY hope of winning is to sweep it out of the small intestine with mechanical action, like a broom sweeping out debris. This is what the Migrating Motor Complex (MMC) is all about. MMC refers to the "gut clearing" waves that happen every 45–180 minutes between meals. If the gut clearing is weak, you get trash left over in the gut, i.e., SIBO.
- About half the time, elemental diets do work, but they only work because they partially restore MMC function! Per Pimentel: "I think the elemental diet is working because it is absorbed in the first 3 feet of small bowel. So the latter 12 feet of small bowel do not see food and bacteria die and dramatically reduce in number. You might say "but in the first 3 feet there is all that good elemental stuff". That area is tough for bugs because they get bombarded with acid (kills them). They get bombarded with bile (it's a detergent and kills them) and they get bombarded with enzymes that try to digest them, from the pancreas (which can kill them). Also, If 12/15 feet of small bowel no longer have bacteria (starved out), that's an 80% reduction in bacterial load." But there has to be more going on than this. As noted even the previous point, even if you killed 99.9% of the bacteria this way, it will all come back in just 5 days! So what's going on? Mark wrote, "We did see in a 2003 paper we wrote that when you get rid of SIBO, MMC are halfway normal. Not perfect. So still could use prokinetic in order to stay in remission." In short, when you eradicate the SIBO, your MMC comes back halfway which can keep you from a remission and this remission is even more likely if you take a prokinetic. That's why the Elemental Diet works for some people… kill + partial restoration of MMC.
- Probiotics and prebiotics: Avoid both. Probiotics have mixed results and prebiotics (fiber) is something you want to avoid since it ferments. But like I said, this is fine tuning. I pretty much ignore this myself and there is no symptomatic difference.
- Methane from methanogens can cause constipation. So type of bacteria you have can cause C or D. But since we do not yet have hydrogen sulfide on the breath test, it's still confusing because this gas can cause diarrhea. In short, you can have a normal-looking breath test and D, and be confused; the cause may be the gas you can't (yet) measure
- The new trio "gold standard" breath test that tests for hydrogen, methane and hydrogen sulfide is now available from Gemelli Biotech. They call it "trio-smart" and the third gas is correlated with diarrhea. Here is the URL: www.triosmartbreath.com. It costs $289 and is covered by most insurance plans.
Prucalopride: the best prokinetic
Here's an article on prucalopride: An update on prucalopride in the treatment of chronic constipation describes prucalopride's role in facilitating MMC.
Prucalopride is now FDA approved and now sold as Motegrity. So the FDA has determined that the reports of cancer risk is insignificant.
Pimentel recommends this as THE drug to get for motility. Your ND will never suggest this because the ND isn't licensed to prescribe it! Instead, you'll likely get recommended MotilPro which has 5-HTP so it does work, but has the downside of causing stomach pain in therapeutic doses. This is why you want to go to a GI, and not an ND.
Getting Prucalopride if you are outside the US, Canada, UK, ….
If Prucalopride isn't available in your country, you can likely get it by sending in your prescription to a Canadian Pharmacy where it goes under various brand names like Resolor, Prudac, and DuphaPro.
I highly recommend Mark's Marine Pharmacy in Canada for several reasons: 1) great price, 2) great personal service, 3) very fast email response (e.g., 5 minutes), 4) expedited shipping available, 5) can accept prescriptions from all over the world and ship anywhere, 6) recommendations of others, 7) family owned and operated, 8) serving the community for over 50 years and shipping into the US for the last 20 years, 9) and my personal experience. You can also get it in pharmacies in the UK and elsewhere in Europe. Canada is best/simplest because they can accept prescriptions from a doctor anywhere in the world and the prices are much lower than other areas.
To save money on prucalopride, order the 3-pack of 2mg pills (84 pills) which gives you a discount over buying 1 pack (28 pills). Use a pill cutter to split the pills into 4 pieces (first in half, then split each half); the pills are large enough to be easily cut.
Prucalopride does have lactose, but no need for lactase
I am severely lactose intolerant but get no gas from the prucalopride, probably because of the small amount.
Prucalopride dose amount
You can start at .5 mg per night and adjust based on your results.
Basically there are 3 ways to tell what is an effective dose for you:
- Are your symptoms diminishing?
- Are your stools reasonably soft? That's a good indicator. They shouldn't be like they are barely hanging together, and they shouldn't be hard coming out. Stools should come out nice and easy and be intact. Mark wrote: "You want soft as the best outcome and optimal motility effect."
- Does bloating due to eating a "bad meal" (like baked beans or rich in lactose) fully resolve by morning? Bloating resolution is all MMC. So I've blown myself up and expanded by 2". If you take the right dose 4+ hours after dinner, you should resolve all excess bloating by morning, essentially resetting you back to normal. If you aren't getting a full reset, you should up the dose in .5mg increments.
Mark wrote: "If you're MMC's are perfect (never had bloating) if you swallowed air, the MMC should clear out the air along with the debris as part of cleaning function. If MMC is impaired and somewhat corrected with resolor, it will improve but it is hard to know if the resolor completely restored or just improved the MMC's."
Some people can get efficacy at an even lower dose than .5mg. It all depends on how much of you MMC you recovered after you got rid of your SIBO, and your sensitivity to the drug. Once your SIBO is gone, you should be able to reduce your dose because you'll usually have recovered about half your original MMC.
The first time I took it (.5mg), I had no side effects whatsoever, just a clearly "looser" stool the morning instead of hard pack! I had absolutely none of the "up all night, bathroom every 10 minutes" horror experiences reported by others because I took the recommended dose: .5mg (i.e., 1/4 of the 2mg pill) on an empty stomach.
Note: Resolor can cause diarrhea at higher doses. If you get diarrhea, either you are taking too much drug or not waiting long enough before you swallow the pill. Diarrhea is not a function of MMC. MMC is in the small intestine; diarrhea is the colon.
Prucalopride dose timing
This one is extremely important: ONLY take resolor if you are FULLY FASTED. So at least 4 hours fasting before you take it. If you need to cut short the time, do it on the backend, e..g, fast for 8 hours after taking the pill.
**** If you take resolor if you are not fully fasted , it will make things WORSE ***
Mark wrote:
"If you take Resolor while fasted, it should totally resolve bloating from your dinner. Resolor potently encourages all the motility happening right now. If you are digesting food, that will go faster. If you are fasting, MMC will happen more often."
So in other words, if you take it while not fully fasted, your food will pass down undigested which actually makes things worse.
Per Mark: "So… if you take resolor too soon after a meal, you do not cause cleaning waves (MMCs). You force the food down too fast. Thus the bacteria now have the greatest feast. More bloating and won't work that night. Dinner might have been too close to resolor. I tell my patients if you have a late dinner with friends, either skip that night or set alarm for 1 am and take it then."
Prucalopride side effects
As you increase the dose, your headaches will get worse.
Increase it too much and expect diarrhea.
Manually deflating the air in your intestine
I wondered: can you manually deflate my distention like letting the air out of a tire?
Answer: "No way to do that. Unless you want a venting gastrostomy tube. You do not want a venting gastrostomy tube." I looked it up. He wasn't kidding.
How long will you need to remain on a prokinetic?
Here is the breakdown from Mark:
- 30% of people who respond to antibiotics can go months and not need prokinetics. Some of these people never need anything. Antibiotics and done.
- 30% will need a prokinetic for 1 year or more and be able to stop.
- 30% will need a prokinetic for life.
- 10% do not respond to prokinetics at all. If you get an IBS-smart blood test and have a very high anti-vinculin value, it can be predictive of being in the unlucky 10%. According to Mark, those patients are treated with "combinations of things that partially work in trial and error approach."
Mark wrote me: "I do believe that the anti-vinculin antibody is what determines recovery of MMC. When that diminishes to normal, the MMC will improve. But no data on this published yet." See IBS-smart blood test in this article for more info on anti-vinculin antibody. I was negative so that's a relief.
Gut motility testing
Generally, the simplest way to confirm your gut motility is still viable is if the treatments with prucalopride reduce your symptoms (less bloating), or lead to a lower score on the breath tests.
Another easy way to get confirmation is the presence stomach growling. When I take prucalopride at midnight, and stay fasted for 12 hours, I'll typically have stomach growling around 10am. This is actually a good sign and shows that the MMC is activated!
If you are not making any progress with a prokinetic properly dosed, then it could be time for some more serious tests like checking your gut motility.
Motility testing is no walk in the park. A handful of centers can measure MMC. Pimentel can do it but it's invasive and requires 6 hours with a tube in your nose into the small intestine. Not super fun.
The easier way to measure motility is with a smartPill. I'm doing this now (at day 2) since I've done the CAT scan, MRI, and had an upper endoscopy with biopsy, all of which were inconclusive.
Also, the IFFGD info page on motility testing can direct you to places where you can have your motility measured. There are various methods for measuring gut motility (see this paper and this paper), but the SmartPill seems pretty easy and it measures transit for 5 days.
Breath tests
IMPORTANT: some clinics will test H2 only and use a criteria of HOB (hydrogen over baseline) as the criteria. Avoid this! That's not acceptable today yet it happens because clinics don't upgrade their machines (the original Quintron machines were H2 only and they are expensive to upgrade). Any GI relying on a H2 only test for SIBO is simply going to give you bad advice.
Please get a real test that looks at least the two major gasses: H2 and methane using lactulose (not lactose) as the substrate. That's because methane producing bacteria eats the hydrogen so you can have normal hydrogen but still have SIBO.
If you are at the cutting edge, get a test that looks at all three gases: hydrogen, methane, hydrogen sulfide.
Breath test prep is overkill
With respect to the breath test prep, the whole point is simply to reduce your "baseline" emissions to be as low as possible. This makes the test more sensitive to variations. The purpose of the test is to look at emissions in the first 2 hrs as the substrate makes it way down your small intestine. If you have high emissions to start (from your large intestine), it's just going to be harder to see what you are interested in seeing… how much excess gases are produced over baseline.
The point of the prep is not to introduce any "munchables" for the bacteria so as long as all carbs are fully digestible (minimal fiber), you'll be fine. And butter is fine if you take lactase pills 15 minutes before (if you are lactose intolerant). So you can have white bread, rice, cream of wheat, Special K, oranges, really ripe bananas (green bananas have resistant starch), etc.
Therefore, the breath test diet they tell you to eat is overly restrictive. I confirmed with Mark that all you really need to do to prep for the breath test is eat per Mark's low-fermentation diet for 24 hours before the test, and then fast the final 12 hours before the test. I did just that eating a LFD dinner 12 hours before the test that included butter (with lactase pills), cream of wheat, protein shake (2 scoops of whey+ which is whey isolate), several ripe bananas (ripe bananas have sugar instead of resistant starch), cacao powder, Special K, popcorn with coconut oil and butter, fish oil pills, whole orange, and whole milk w/o lactose. I brushed my teeth in the morning, rinsed with water. My baseline score was 0 H2 and 3 CH4 which is excellent (and far better than the 0, 16 values I had when I followed the prep instructions exactly and had more SIBO at that time).
If you did the proper prep for the test (fasting, limiting diet), then your baseline should be 10ppm or lower for H2 and 5ppm or lower for methane.
Interpreting the breath test results
H2 and methane are ONLY emitted by bacteria.
To interpret your test, download Mark's paper in #3 below so you see what normal and SIBO positive breath tests look like. The "criteria" used by doctors is rather simplistic. Compare your graphs with those references and you'll be way ahead of the game.
SIBO criteria: Generally, any high reading on an absolute scale is cause for concern, including baseline readings and those taken at the first test. A normal breath test will have the H2 gradually rising (ebb and flow) to generally 25ppm or less and the CH4 remaining at 5ppm or less.
SIBO criteria per Mark's paper:
- Normal: lack of excessive methane production or an early rise in hydrogen excretion within 90 min of the test
- H2 SIBO: Hydrogen production rises by more than 20 ppm within 90 min
- Methane SIBO: Methane levels of more than 10 ppm
The most expensive tests are in-clinic. For example, Stanford charges you $550 per test. That is your out of pocket after they adjust for insurance!
The cheapest test I've found is straight from the manufacturer: https://www.breathtests.com/patients which sells for $150 and is right from the manufacturer. You get 10 tubes: 1 for the reference, then tubes for every 20 minutes for the next 3 hours (so 3 per hour x 3 hours). This is what I'd recommend.
To get the lactulose (10g of lactulose is the standard dose), the cheapest/easiest way is order a bottle separately, e.g., from a Canadian pharmacy or if you are in the UK, you can simply walk into a pharmacy and speak to the pharmacist. This avoids having to have a prescription every time you order a breath test. It will probably come as 3.3g/5ml. So, if it is not pre-packaged for you, you will need to pour 15ml volume of lactulose solution to get the 10g dose. Also, even though it can't be digested by your body, you can get a severe allergic reaction to it, which is probably why you need a prescription to get it.
If you are a bit clever, you can use the standardized test in a non-standard way to monitor your progress on antibiotics by ordering the standard kit for $170 and then instead of doing it per instructions (diet restriction prep, the substrate, and testing every 20 minutes), you ditch the substrate and the prep, and do it daily, fasted, in the morning, after brushing your teeth and rinsing. That way you can track daily progress while on an antibiotic combo or while you are on the prokinetic. Since you'll get only 9 tubes and they don't know when you took the samples so take samples daily during the final 9 of your antibiotic treatment or once every 3 days while on the prokinectic (since it works slower). If there is any drop in your numbers, it will only show up in the last half of your treatment. In my case since I've got methane SIBO, I'm looking for a fasted/no substrate reading of 5 ppm of methane or less. Some people get to zero. Now you have a very nice record of the antibiotic treatment effectiveness (or lack thereof) which can help you to decide whether it was working at all, whether to continue it, and it only cost you $170 for the entire daily monitoring; now that's a deal!
The Quintron machine is the gold standard for breath tests, but there will be a new machine out in 2019 that analyzes all three gases that are relevant for SIBO: hydrogen, methane, and hydrogen sulfide. You'll be able to get a home test kit starting in May 2019 from a new company (will be announced in Feb 2019) and see all 3 gases. So this will be the new "gold standard" for breath testing.
My journey with SIBO
My stomach has been bloated for 10 years consistently, so I didn't think this was going to be a quick fix.
At my behest, my GI ordered a SIBO breath test which I took at Stanford on 12/21/18. Note elevated baseline CH4… an ominous sign! Just 20 minutes later when the first results came in, I knew I had a severe case of methane SIBO!
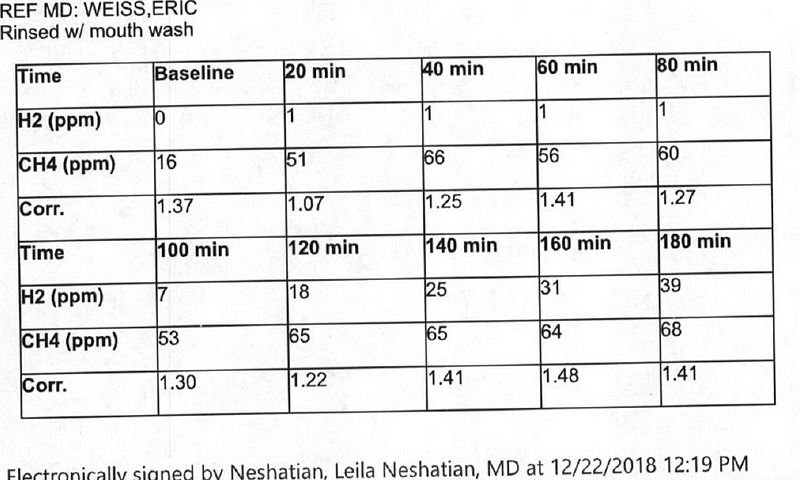
1/11/19: Since I'm methane SIBO, Pimentel suggested best course of action would be 14 days of Rifaximin @ 550mg/pill)+ Flagyl (aka Metronidazole)@250mg/pill. You take 3 pills/day, spaced 8 hours apart so you get constant coverage. 14 day supply of both pills. Eat a normal diet.
1/25/19: At the end of the 14 days, I was just as bloated as I was when I started the antibiotics. I was in the UK at the time and met with a doctor at Roodlane Medical and got him to write a prescription for a box Resolor for me (28 2mg tablets) which I started taking at .5mg per night (using a pill cutter), and then later upped it to 1 mg per night. I could see my bloating start to diminish gradually. I take the pill >4 hours after my last bite of food, and then fast completely for the next 12 hours (no pills, no vitamins, no coffee, nothing except water).
2/13/19: SIBO lactulose breath re-test at Stanford to see where I am now. Results for H2, CH4 were (every 20 minutes):
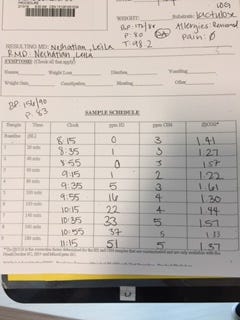
Bottom line:
- This is a "normal" breath test (see Mark's criteria above)!
- It basically took me 14 days on antibiotics + only 7 2mg Resolor pills (taken over the next 2 weeks as .5mg or 1mg) to completely get rid of the SIBO that I've probably had for 10 years. So < 30 days of treatment!
- Symptoms can be deceiving! You cannot tell you got rid of the SIBO without the breath test! I cannot stress this enough. Had I gone by my symptoms (bloating), I would have thought my treatment was useless and would have repeated it; in reality my breath test is now normal so I was successful. Beware: there are doctors who think you can judge by the symptoms; you'd want to steer clear of such advice.
- I probably didn't need to go as far as I did on the Resolor (to 1mg). Dropping back to .5mg is probably sufficient at this time. It's really tough to tell the proper dose: stool softness isn't an indicator.
- Clearly, my stomach distention was only minimally caused by SIBO since the SIBO is gone. There is something else that is causing the consistent bloating. Still a mystery! There is a nice checklist for bloating here. I ruled out my CPAP machine (you can lower pressure or use bipap) and it was not a reaction to metformin which I take for diabetes. And it might be a few other things. You basically have to use clues to guide you. Mark wrote: "I have seen some patients with a lot of distension from CPAP. Can take hours to go down for some people but should go down throughout the day." That is as long as your MMC is working!
Nothing resolved my distention so Mark suggested I see Linda Nguyen at Stanford who is a motility specialist. Best suggestion ever! Linda went through my history and symptoms. Then she listened to my stomach. "Sounds pretty quiet," she said. So that was confirmation of her hypothesis. She then wrote me up for:
- CT abdomen and pelvis to assess for progression of retroperitoneal adenopathy
- MR enterography to evaluate for an small bowel obstruction and small bowel motility
- Upper GI endoscopy with biopsy of the small bowel and stomach to evaluate for presence of an infiltrative disorder
So two different scans (to see if there are any lumps, bumps, and a second scan for blockages (using contrast), and a upper GI tract endoscopy. If I pass the tests, then I get a smart pill. You never want to take a smart pill before the imaging tests because if the passages aren't clear, the pill gets stuck and it requires emergency surgery to remove the pill. That would NOT be fun.
Therefore I am still looking for the underlying cause of my SIBO. And you should ALWAYS look for the underlying cause… SIBO is just a symptom of something bigger.
Per my GI, my bloating isn't air. It was food stuck in my intestine. This totally explains why big meals always bloat me! And why eating late at night means I'm more bloated in the morning. And it explains why when I did my DXA scan, the technician said, "that's odd, you have way more lean mass in your abdomen than is possible for someone of your weight/body fat %." Now it's all coming clear. That was food that showed up as lean mass. If it were air, it wouldn't have registered. So that mystery is FINALLY (almost) solved.
So will I be able to get a flat stomach? It's about 50% chance right now; it depends on the cause which we'll find out soon after all the tests are done.
It turns out that problems in the small intestine have fewer treatment options. Generally treatments are drugs and/or surgery. She thinks my motility may have been harmed from chemo treatments 10 years ago when I was diagnosed with Waldenstrom's (an incurable blood cancer), because I've had distention for 10 years and cancer for 10 years. A little too coincidental.
I've done the IBS-smart test (described elsewhere in this article) and that was negative.
- I still have a motility problem so keeping the prokinetics and the discrete eating style is still a good idea. Want to prevent a relapse and .5mg is a tiny dose of the drug.
- I validated I distend 2" after eating certain foods. Not clear which ones since I had a huge combo and I thought my lactase dosing was right. So my bloating is food triggered for sure.
- CPAP didn't change my distension from bedtime to morning so eliminated that. I also discontinued for a night and it made no difference.
- Stopping Metformin make for several days no difference in my fasted distension measurement so it wasn't that.
- I can inflate by 2" even after being careful to avoid lactose.
- So until we figure out the cause, I'll take the Resolor and be diligent on the lactase pills.
Misc
If you have SIBO, you should get an IBS-smart blood test. It tells you 3 things:
- why you have the overgrowth, what the mechanisms are, and a possible cause.
- The higher they are, the worse the patient is. So tells you severity
- Tells you if the treatments in the future will actually be making things better.
The GI Map has mixed reviews with some people swearing by it and others saying it is expensive and useless. Pimentel is in the latter group and doesn't use it at all.
SIBO Required Reading List
- This article since it contains the latest drugs and tricks
- Low-Fermentation Diet (LFD) guide (written by Mark)
- Mark's paper
How to Test and Treat Small Intestinal Bacterial Overgrowth: an Evidence-Based Approach (Mark is a primary author). This is going to cost $40 (if you download it legally) but it is required reading. Table 1 is super helpful because a lot of people can't tolerate prucalopride. Table 1 lists other options. I read the paper before I talked to Mark, and it's only then (in talking to him) that you get added insights like "SIBO can be completely cured with just a prokinetic; the drugs just make it go faster". This makes total sense as you can't get SIBO without having a motility problem… fix the motility, your SIBO is gone. You can also read the paper for free here, but that would be a copyright violation. The paper lists underlying causes of SIBO and shows plots showing normal and abnormal breath test results. - SIBO conference recommendations: reasonable options
- Allison Siebecker's SIBO website: a really great objective resource. Of the SIBO websites I've seen, I thought this site was, by far, a real standout because it correlated almost exactly (things change over time such as the Flagyl advice) to advice from Pimentel and published papers about SIBO.
- Sibo Survivor website: Has a lot of good info especially explaining the MMC. Well organized
- Mark's book: A new IBS solution
Other SIBO-related articles of interest
Is GERD caused by SIBO?
If true, PPI's are actually detrimental (which is contrary to established thinking).
FAQ
Quick answers to questions about the content.
- One of the reasons I wrote the article is to correct previously published info. For example, I was surprised when Mark said Flagyl works better then neomycin because his published papers talked about neomycin but that's because it is better studied, but his clinical experience is that Flagyl performs better than neomycin for methane SIBO. You only need Flagyl if you have high methane emissions.
- I am just finishing the antibiotic regimen Mark recommended and it did almost nothing for my bloating after 14 days. I'm on Resolor at 1mg at night and it is a slow road, but I can clearly see some progress.
- There are no food restrictions while taking the antibiotics. You are actually best off eating "normally" since the bacteria is easier to kill when they are dividing. And after you get rid of SIBO, you can eat normally as well: use the prokinetic and eat discrete meals.
- I realized the "daily testing trick" recently. There is no reason it won't work… The methane will stay in the tube forever (we know greenhouse gasses stay in the atmosphere for 1,000 years).
- There are other prokinetics that have impact for MMC. Mark's experience is prucalopride works best. In particular, he does not recommend taking Reglan due to the very serious potential side effects. Some other alternatives are listed in the paper in the table at the end.
- All prokinetics will take a while (3 weeks or more) to see impact. It's a slow grind! And progress is going to be slower at the beginning because there is simply more debris to clean out and you are basically cleaning out at a fixed rate.
- If you are anywhere in the world, you can get prucalopride from any Canadian pharmacy.
- IBS-C and IBS-D are "generic diagnoses" while SIBO is a very specific condition. Both IBS-C and IBS-D can be caused by SIBO, but there can be other underlying causes as well.
- Bloating is very common for methane-dominant SIBO. There is no guarantee you'll get rid of you bloating if you get rid of your SIBO (because there can be multiple causes of your bloating). Getting rid of SIBO is simply "one down" in you checklist. So if you have bloating, get to a near zero breath test. Then if still bloated, look for other causes.
- If you have SIBO, you could have constipation, diarrhea, or regular bowel movements. In all cases, prokinetics are recommended. The only difference in treatment is whether your SIBO it is hydrogen or methane dominant: if hydrogen dominant, then Flagyl is omitted from the antibiotic regimen. Hydrogen dominant is often associated with IBS-D symptoms, methane dominant is often associated with IBS-C symptoms. In my case, I have severe methane SIBO, but I do 4 bowel movements a day. Go figure.
- If your physician is giving you wacky advice (e.g., they say "trust me"), you have several options:
1. There is a list of SIBO doctors in this article.
2. Seek out a GI who at least has an open mind and educate them about this article and have them read the "SIBO required reading list" above. Then discuss options.
3. Read the materials yourself, and find a physician who will write a prescription for the needed drugs. This is pretty much the best way, become your own expert. With a little work, you'll know most everything important you need to know about SIBO. Your doctor won't do all this; he has to handle too many issues to focus on a single one; but you have a much higher vested interest in the problem. For most GI's, you're going to be educating them. Look at it as a public service. Pimentel was the pleasant exception where he knows >100x more than whatever I could uncover through a lot of reading of technical papers. - I was wondering if the reason antibiotics fail sometimes is due to gut motility issues. Answer: "No. Because rifaximin will not be absorbed so will just slowly go through."
- If you want to save this article locally: at the of the post are 3 dots. Tap then tap save link. You can create categories for the posts you save like filing in a filing cabinet.
SIBO doctors
Dr. Elena Ivanina NYC
Dr. Andrew Wong Washington DC metro area
Dr. Satish Rao Augusta GA
Dr. Michael Ruscio Bay Area California
Dr. Kenneth Brown Plano Texas
Dr. Sandberg Lewis and associates in Portland Oregon
Dr Preet Khangura, SIBO specialist who trains other doctors in SIBO, Canada, British Columbia
See also the longer list of SIBO doctors
IMPORTANT: If you liked the article, please clap multiple times using the hand icon just below this and to the left as it helps raise the visibility so others can benefit from Mark's advice.
By Steve Kirsch on January 23, 2019.
How To Get Rid Of Sibo
Source: https://www.skirsch.io/sibo/
Posted by: reeselationd.blogspot.com
0 Response to "How To Get Rid Of Sibo"
Post a Comment